Maca Root for Women: Hormones, Energy & What Science Says

If you’ve looked into natural hormone support, you’ve probably come across maca root. You’ve also probably seen it described in two completely contradictory ways: as a “hormone-balancing” superfood with centuries of traditional use, and as an overhyped supplement with weak evidence. Both descriptions miss what the clinical research actually shows.
Four randomized controlled trials in perimenopausal and postmenopausal women found measurable improvements in estradiol levels, FSH reduction, and relief of menopause symptoms with daily maca supplementation. And here’s what makes maca genuinely interesting: it doesn’t contain plant estrogens, doesn’t act on estrogen receptors, and doesn’t raise or lower hormone levels directly. It works further upstream — on the hypothalamus and pituitary gland — and that distinction changes how it should be used, by whom, and at what dose.
This guide covers the clinical evidence, the mechanism, which type of maca matters for women specifically, and who should and shouldn’t be taking it.
💡 Quick Answer: Maca Root for Women
Maca root (Lepidium meyenii) supports hormonal balance in women by acting on the hypothalamic-pituitary-ovarian (HPO) axis — not by adding or mimicking hormones. Clinical trials in perimenopausal and postmenopausal women show increases in estradiol, reductions in FSH, improved libido, and relief of menopause symptoms at 2–3.5g/day of gelatinized maca over 2–4 months.
- 📋 Written by Ethan Cole, Nutrition Expert | Meet Ethan →
- ✔ Verified against third-party Certificates of Analysis (COAs), current Amazon listings, and 2025–2026 clinical research
- 📅 Last Updated: May 2026
⚠️ This article does not constitute medical advice. If you manage blood sugar with prescription medication, discuss any supplement changes with your healthcare provider before making them.
⚠️This article contains affiliate links. If you purchase through our links, we may earn a small commission at no extra cost to you. See our Affiliate Disclosure for details.
Why Most Maca Articles Get the Mechanism Wrong

There’s a fundamental misconception about how maca works that leads to misuse, disappointment, and unfair dismissal of a genuinely interesting herb.
Maca is not a phytoestrogen. It doesn’t contain plant hormones. It doesn’t bind to estrogen receptors. A 2008 study by Brooks et al. specifically tested whether maca’s benefits in postmenopausal women were related to estrogen or androgen activity — measuring serum E2, FSH, LH, testosterone, and SHBG before and after supplementation. None of those hormones changed. And yet the women in the maca group still showed significant improvements in psychological symptoms and sexual dysfunction compared to placebo.
So how does it work?
The HPO axis explanation: Maca’s bioactive compounds — particularly macamides, macaenes, and plant sterols — appear to act on the hypothalamus and pituitary gland, supporting the body’s own hormonal regulation system. The hypothalamic-pituitary- ovarian (HPO) axis is the master control loop for sex hormone production: the hypothalamus signals the pituitary, which signals the ovaries, which produce estrogen and progesterone.
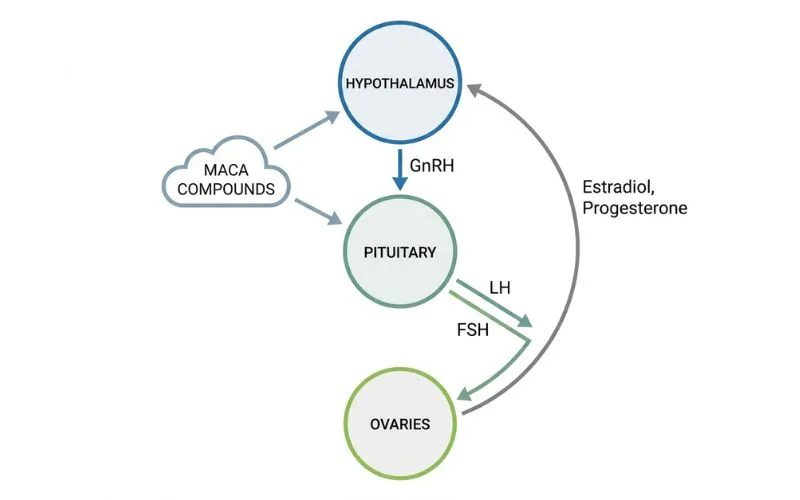
When this axis is dysregulated — as happens during perimenopause when ovarian function begins to decline — maca’s upstream action on the hypothalamus and pituitary appears to help the system communicate more effectively, stimulating more balanced output from the ovaries. This is fundamentally different from taking exogenous estrogen or consuming phytoestrogens that mimic it.
Why this matters: because it means maca’s hormonal effects are regulatory, not additive. It doesn’t simply push estrogen higher. It helps the body’s own system find a more functional equilibrium. This also explains why maca works differently in different hormonal contexts — and why the dosage and form you use matters.
What the Clinical Research Actually Shows

Trial 1 — Meissner et al. 2006 (Perimenopausal Women)
A four-month double-blind, crossover, randomized pilot trial enrolled 20 perimenopausal women aged 41–50. They received pre-gelatinized Maca-GO at 2g/day in two divided doses. Monthly blood tests tracked estradiol (E2), FSH, LH, progesterone, cortisol, ACTH, thyroid hormones, and minerals.
Results after two months of maca supplementation:
- Estradiol (E2) increased significantly
- FSH decreased (reduced ovarian stress signaling)
- Cortisol levels dropped
- Kupperman Menopausal Index scores improved — particularly hot flashes and night sweats
- Bone density markers improved
This trial is significant because it used objective hormone measurements — not just self-reported symptom surveys — and because it was conducted in perimenopausal women whose ovaries still had functional capacity. Maca’s effect here appears to be supporting ovarian output during a period of declining but not absent function.
→ 🔗 Meissner et al. 2006 (Perimenopausal Women) – Primary perimenopausal RCT citation
Trial 2 — Meissner et al. 2005/2006 (Early Postmenopausal Women)
A larger double-blind, randomized, placebo-controlled multicenter trial enrolled 168 early postmenopausal women (age >49, FSH >30 IU/ml, E2 <40 pg/ml) across five sites. Women received 2g/day of gelatinized Maca-GO for 3–4 months.
Results:
- E2 (estradiol) and progesterone both increased
- FSH decreased
- Greene Menopausal Index scores improved significantly
- Symptom relief reported by 83% of women within 21 days for hot flashes, night sweats, mood swings, and sleep disruption
The PMC reference for this study is PMC3614576 and PMC3614647.
Trial 3 — Brooks et al. 2008 (Psychological + Sexual Function)
This trial is the most clinically illuminating for understanding maca’s mechanism. Postmenopausal women received maca supplementation and showed significant improvements in psychological symptoms and sexual dysfunction scores — but with no change in serum E2, FSH, LH, or SHBG.
The implication: maca’s benefits for mood, libido, and symptom relief in postmenopausal women appear to come through a non-estrogenic pathway — likely direct neurochemical effects of macamides and macaenes on the central nervous system, rather than through hormone level changes.
This is why maca can work at different stages of hormonal life: perimenopausal women show hormone-level changes; postmenopausal women show symptom changes without hormone changes. Different mechanisms, same direction.
→ 🔗 Brooks et al. 2008 – No change in E2/FSH/LH despite symptom improvement
Trial 4 — Systematic Review, Lee et al. 2011 (PMID: 21840656)
A systematic review of all randomized clinical trials on maca for menopausal symptoms identified four RCTs meeting inclusion criteria. All four showed favorable effects using the Kupperman Menopausal Index and the Greene Climacteric Score. The authors noted the evidence base was promising but called for larger, longer trials before definitive conclusions.
Maca Root Clinical Data Summary
| Study | Participants | Dose | Duration | Key Outcome |
|---|---|---|---|---|
| Meissner 2006 (PMC3614596) | 20 perimenopausal women 41–50 | 2g/day Maca-GO | 4 months | ↑E2, ↓FSH, ↓cortisol, ↓menopausal symptoms |
| Meissner 2005 (PMC3614576) | 20 early postmenopausal women | 2g/day gelatinized | 2–8 months | ↑E2, ↑progesterone, ↓FSH, symptom relief |
| Meissner 2006 multicenter (PMC3614647) | 168 early postmenopausal women | 2g/day Maca-GO | 3–4 months | 83% reported symptom relief within 21 days |
| Brooks et al. 2008 | Postmenopausal women | 3.5g/day powder | 6 weeks | ↑libido, ↓sexual dysfunction, ↓depression — NO change in E2/FSH/LH |
| Lee et al. 2011 (PMID: 21840656) | Meta-analysis of 4 RCTs | Varied | Varied | All 4 RCTs showed favorable menopausal symptom effects |
Maca Root Benefits for Women: What’s Supported
1. Perimenopausal Symptom Relief
The strongest evidence for maca is in perimenopausal and early postmenopausal women. Hot flashes, night sweats, mood swings, and sleep disruption all improved in multiple RCTs. The Meissner multicenter trial reported that 83% of women experienced relief within three weeks — a notably fast onset for an herbal intervention.
2. Libido and Sexual Function

Maca’s libido effects appear in multiple contexts. A trial in postmenopausal women showed significant improvement in sexual dysfunction measures at 3.5g/day over six weeks. A separate study found maca helped restore libido in women taking SSRI antidepressants — a notoriously difficult pharmacological problem where no natural intervention shows reliable results. Critically, these benefits occurred without changes in sex hormone levels, suggesting a direct neurochemical action via macamides that don’t require hormonal mediation.
3. Energy and Stamina

Traditional Andean use of maca as an energy food is supported by its nutrient profile: maca contains significant amounts of iron, calcium, zinc, and magnesium, along with amino acids and complex carbohydrates. It has been used for centuries by Andean populations at altitude where physical demands are high. Modern supplement users commonly report improved sustained energy — though controlled energy trials in women specifically are limited. The cortisol reduction seen in the Meissner 2006 trial may contribute to energy improvement through reduced adrenal load.
4. Mood and Depression
A small randomized placebo-controlled study of 29 Chinese postmenopausal women found that 3.3g/day of maca for six weeks produced significant reductions in depression scores compared to placebo. This aligns with maca’s proposed effect on HPO axis regulation — depression in perimenopause is often directly driven by hormonal dysregulation, and interventions that stabilize the hormonal signaling loop tend to improve mood as a downstream effect.
5. Bone Density Support
Red maca specifically has shown promise for bone density in animal studies and limited human data. The Meissner 2006 perimenopausal trial found improvements in bone density markers alongside the hormonal changes. This is mechanistically coherent: estrogen plays a key role in bone maintenance, and anything that supports endogenous estradiol production during the perimenopausal window will likely have secondary bone-protective effects.
The 3 Colors of Maca: Which One Is for Women?
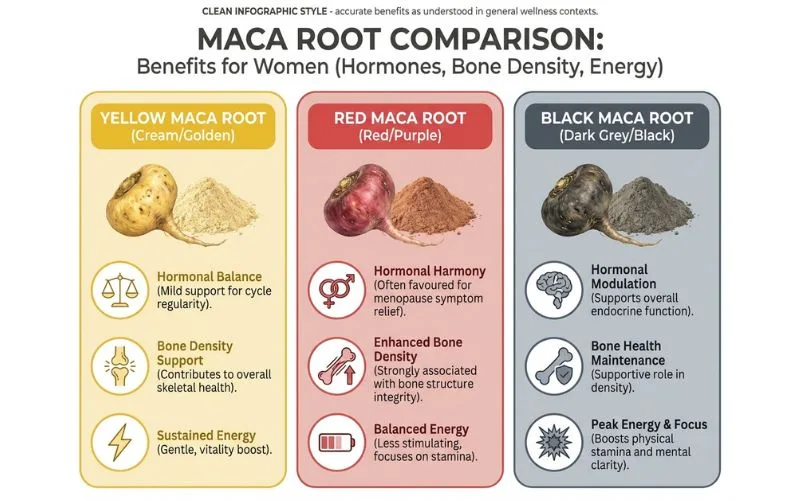
Most people don’t realize that “maca” refers to multiple phenotypes of Lepidium meyenii with meaningfully different phytochemical profiles. The color of the root isn’t just aesthetic — it correlates with different bioactive compound concentrations and different clinical applications.
| Maca Color | Primary Compounds | Best For (Women) | Evidence |
|---|---|---|---|
| Yellow Maca | Balanced macamides + macaenes | General energy, mood, libido, perimenopause | Most studied; used in majority of RCTs |
| Red Maca | Higher glucosinolates, flavonoids | Bone density, hormonal balance, post-menopause | Animal studies + limited human data show bone-protective effect |
| Black Maca | Highest macaene concentration | Athletic performance, cognitive function | Stronger evidence for men; less studied in women specifically |
For most women: Yellow maca is the default clinical choice — it’s what most RCTs used, and it covers the broadest range of goals: energy, libido, menopause symptoms, and mood. Red maca is a reasonable secondary choice for postmenopausal women concerned specifically about bone density, potentially stacked alongside yellow.
Maca for Women at Different Life Stages
Maca’s benefits and the appropriate dose vary depending on where you are hormonally. Using it the same way at 32 and at 52 misses important nuance.
Reproductive-Age Women (25–42)
In women with regular cycles, maca’s primary benefits are energy, libido, mood stability, and stress resilience. At this stage, the ovaries are fully functional — maca’s HPO axis support maintains balance rather than restoring declining function. The evidence for hormone changes in this population is less robust than in peri/ postmenopausal women; the main clinical outcomes here are subjective (energy, mood, libido).
Dosage for reproductive-age women: 1.5–2g/day of gelatinized yellow maca, taken with food. This is lower than perimenopausal doses because the goal is maintenance rather than restoration.
Important: Maca may alter menstrual cycle timing in some women. This is generally in a normalizing direction for women with irregular cycles, but it’s worth tracking when you first start.
Perimenopausal Women (40–52, irregular cycles)
This is where the clinical evidence for maca is strongest. Perimenopause is defined by fluctuating hormone levels as ovarian function begins to decline — and this is precisely the stage where maca’s HPO axis modulation appears to have the greatest impact. The Meissner 2006 perimenopausal trial (women aged 41–50) showed the most significant hormone marker changes of any maca study.
Dosage for perimenopausal women: 2–3g/day of gelatinized yellow maca in two divided doses (with breakfast and lunch). Allow 4–8 weeks for measurable symptom improvement.
Postmenopausal Women (12+ months post-period)
After menopause, the clinical picture shifts. The Brooks 2008 trial showed maca helped postmenopausal women without changing hormone levels — meaning the benefits come through a different pathway at this stage. The focus here is libido, mood, and energy rather than hormonal restoration.
Dosage for postmenopausal women: 3–3.5g/day of gelatinized maca (matching the Brooks and postmenopausal Meissner trial doses). Red maca may be added for additional bone density support.
→ 🔗 NIH Office on Women’s Health — perimenopause overview
Gelatinized vs. Raw Maca: Why Form Matters
This distinction matters more than most buyers realize, and most supplement labels don’t explain it clearly.
Raw maca powder: The dried, ground root. Contains the full phytochemical profile but also contains starch and enzyme inhibitors that can cause GI discomfort (bloating, gas) in some people. Requires higher doses to achieve clinical-level effects because bioavailability is lower.
Gelatinized maca: Raw maca that has been cooked and processed to remove starch and enzyme inhibitors. The result is easier to digest and more concentrated — a 1:1 ratio between gelatinized and raw powder equates to roughly 4:1 in terms of active compound density. This is the form used in all major clinical RCTs.
Verdict: Use gelatinized maca. It’s what the research used, it’s more bioavailable, and it’s easier on digestion. “Raw maca” is not a superior product — it’s just less processed, which in this case is a disadvantage.
Maca Root vs. Ashwagandha for Women: Which Should You Choose?
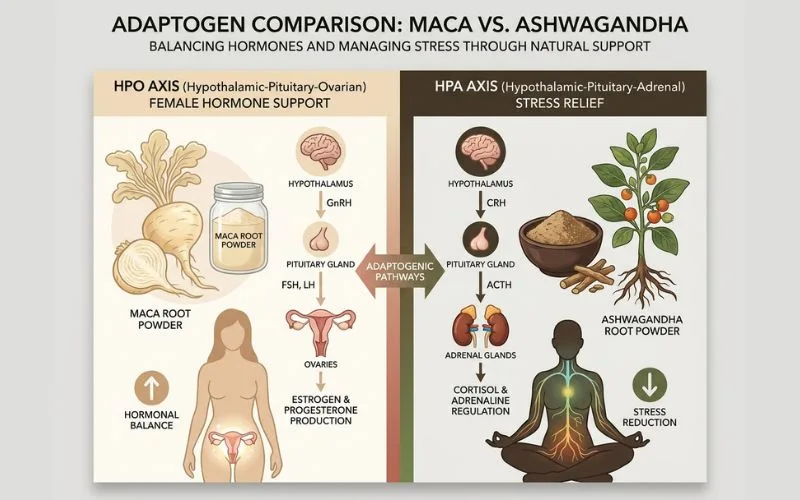
Both are popular women’s wellness adaptogens but work through different mechanisms and suit different goals.
| Factor | Maca Root | Ashwagandha (KSM-66) |
|---|---|---|
| Primary mechanism | HPO axis modulation (hypothalamus-pituitary) | HPA axis (cortisol suppression via GABA) |
| Hormonal effect | ↑E2, ↓FSH in perimenopausal women | No direct sex hormone effect |
| Best for | Libido, perimenopause, energy, bone density | Sleep, anxiety, brain fog, chronic stress |
| Menopause symptoms | Moderate-strong evidence (4 RCTs) | Moderate evidence (1 RCT, 2021) |
| Cortisol | Moderate ↓ (Meissner 2006) | Strong ↓ (~27–28%, KSM-66 trials) |
| Libido | Strong evidence (multiple trials) | Less direct evidence |
| Phytoestrogen | ❌ No | ❌ No |
| Safe to combine | ✅ Yes | ✅ Yes |
| Time to results | 4–8 weeks | 4–8 weeks |
| Best form | Gelatinized powder | KSM-66 or Sensoril extract |
| Taste | Earthy, nutty, malty | Bitter, earthy |
Practical takeaway: These two work well together. For perimenopausal women, a combination of maca (for HPO axis and libido) and ashwagandha (for cortisol and sleep) addresses the two most common underlying issues simultaneously. See our full ashwagandha for stress guide for dosage details on combining them.
Common Mistakes Women Make With Maca Root
1. Using raw maca powder from the grocery store The dried raw maca chips or powder sold at health food stores are not the same as the gelatinized maca extract used in clinical trials. Bioavailability is lower, GI discomfort is more common, and you’ll likely need 4–5g/day to approach clinical-level effects. Gelatinized capsules are a better investment.
2. Expecting results in the first two weeks The Meissner multicenter trial showed 83% of women reporting symptom relief within three weeks — but that’s for active symptoms like hot flashes, not for hormonal marker changes, which took two months to register on blood tests. Give maca at least six to eight weeks before concluding it isn’t working.
3. Not adjusting dose for life stage Taking a reproductive-age dose (1.5g/day) when you’re perimenopausal and need the full 2–3g/day used in RCTs is one of the most common reasons women don’t see results. Dose matters here. Match it to your situation.
4. Taking it at night Maca supports energy and cognitive clarity through its adrenal and HPO axis effects. Several users report difficulty sleeping when they take it in the evening. The clinical protocols all used daytime dosing with meals. Stick to morning and midday dosing.
5. Ignoring the thyroid caution Maca is a glucosinolate-containing crucifer (same family as broccoli, kale, and cabbage). High-dose glucosinolate intake can interfere with thyroid iodine uptake in people with thyroid conditions. If you have hypothyroidism or are on thyroid medication, discuss maca supplementation with your doctor before starting. Cooking (which gelatinization approximates) degrades glucosinolates, which is another reason gelatinized is safer than raw for thyroid-sensitive individuals.
Who Should NOT Use Maca Root
- Women with active, hormone-sensitive cancers: Maca doesn’t act as a phytoestrogen, but given the upstream HPO axis effects, caution and oncologist approval are warranted.
- Women with thyroid conditions: See glucosinolate note above. Use gelatinized form if cleared by your doctor, and start at low dose.
- Pregnant or breastfeeding women: Insufficient safety data. Traditional Andean use suggests it’s been used during pregnancy, but modern clinical evidence for safety in pregnancy does not exist. Avoid until postpartum.
- Women on SSRIs for mood (not libido): The SSRI-maca trial showed libido benefits without affecting antidepressant efficacy, but if your SSRI dose is carefully calibrated, introducing an HPO-modulating supplement warrants a conversation with your prescriber.
FAQ — Maca Root for Women
Does maca root balance hormones in women?
Clinical trials in perimenopausal and early postmenopausal women show that maca increases estradiol and reduces FSH — two markers of improved hormonal balance — at 2g/day of gelatinized maca over two months. However, maca doesn’t directly contain or mimic hormones. It works through the HPO (hypothalamic-pituitary-ovarian) axis, supporting the body’s own hormonal regulation. In postmenopausal women, hormone levels may not change but symptom scores still improve, suggesting additional non-hormonal mechanisms.
How long does it take for maca root to work for women?
For active menopause symptoms like hot flashes and night sweats, some women report improvement within two to three weeks. For objective hormone marker changes (E2, FSH), the Meissner trials measured significant shifts at two months. For libido and mood, most clinical trials ran six to eight weeks. A fair evaluation period is eight weeks of consistent daily use before drawing conclusions.
What is the best maca root for women’s hormones?
Gelatinized yellow maca — the form used in most RCTs — is the best-supported choice for women’s hormonal health. Yellow maca covers the broadest range of goals: energy, libido, hot flashes, mood, and perimenopause. Red maca is an additional option for postmenopausal women concerned about bone density, as it shows higher glucosinolate and flavonoid content associated with bone-protective effects in animal models.
Can maca root help with perimenopause?
Yes — the clinical evidence for maca in perimenopause is among the strongest of any herb in this category. A double-blind crossover RCT in women aged 41–50 found measurable increases in estradiol, reductions in FSH and cortisol, and improvements in the Kupperman Menopausal Index after two months of 2g/day gelatinized maca. For women in the perimenopausal window with fluctuating rather than absent ovarian function, maca’s HPO axis support appears to be particularly effective.
Is maca root a phytoestrogen?
No. Maca does not contain plant estrogens and does not bind to estrogen receptors. The Brooks 2008 clinical trial specifically measured E2, FSH, LH, testosterone, and SHBG before and after maca supplementation and found no changes in any of these markers. This makes maca meaningfully different from herbs like red clover and soy isoflavones, which do act on estrogen receptors and carry different safety considerations for hormone-sensitive conditions.
Can I take maca root with ashwagandha?
Yes — they work through different mechanisms and can be taken together safely. Maca primarily modulates the HPO (ovarian) axis and supports libido and hormonal balance. Ashwagandha primarily modulates the HPA (adrenal/cortisol) axis and supports sleep and stress resilience. The practical combination for perimenopausal women is maca with breakfast (energy, hormonal support) and ashwagandha before bed (sleep, cortisol recovery).
What is the right dose of maca for women?
Clinical trials used 2–3.5g/day of gelatinized maca. For reproductive-age women seeking energy and mood support, 1.5–2g/day is a reasonable starting dose. For perimenopausal women targeting hormone balance and symptom relief, 2–3g/day in divided doses (morning and midday) matches the RCT protocols. For postmenopausal women, the Brooks trial used 3.5g/day. Always use gelatinized form for better bioavailability and less GI discomfort.
Can maca root help with PCOS?
Direct RCT evidence for maca in PCOS is very limited. Maca’s potential relevance is through HPO axis regulation and the energy/adrenal support that may help with cortisol-driven symptoms common in PCOS. However, given that PCOS involves complex hormonal dysregulation, maca should be approached as a supportive addition to a broader protocol — not a primary intervention — and discussed with your gynecologist or endocrinologist.
Does maca root help with libido in women on antidepressants?
There is direct clinical evidence for this specific application. A double-blind, placebo-controlled trial (Dording et al.) found that maca root significantly improved sexual dysfunction symptoms in women taking SSRI/SNRI antidepressants, which commonly cause libido suppression as a side effect. At 3g/day, maca supported libido restoration without interfering with antidepressant efficacy — a clinically meaningful outcome given how common this SSRI side effect is.
Is maca root safe for long-term use?
Maca has been used as a staple food in the Peruvian Andes for centuries, which provides a strong historical safety record. Clinical trials lasting up to 4 months show no significant adverse effects at doses of 2–3.5g/day. The most common reported side effects are mild GI discomfort (particularly with raw maca) and occasional altered menstrual timing in reproductive-age women. The glucosinolate content is a relevant caution for thyroid conditions. For most healthy women without thyroid issues or hormone-sensitive cancers, daily maca use at clinical doses appears safe.
How to Take Maca Root: A Practical Protocol by Life Stage
For Reproductive-Age Women (25–42)
- Dose: 1.5–2g/day of gelatinized yellow maca powder
- Timing: Morning with breakfast (in smoothie or with water)
- Form: Gelatinized capsules OR powder in smoothies
- Duration: Daily ongoing; cycle if preferred (5 days on, 2 off)
- Goal: Energy, libido, mood stability, stress resilience
For Perimenopausal Women (40–52)
- Dose: 2–3g/day of gelatinized yellow maca
- Split: 1g with breakfast + 1–2g with lunch (avoid evening)
- Add: 300–600 mg ashwagandha at night for sleep and cortisol
- Duration: Continuous; evaluate at 8 weeks
- Goal: Estradiol support, FSH reduction, hot flash relief, libido
For Postmenopausal Women (52+)
- Dose: 3–3.5g/day gelatinized yellow OR red maca
- Split: 1.5g morning + 1.5g midday
- Consider: Adding red maca 1g/day for bone density benefit
- Duration: Continuous
- Goal: Libido, mood, energy, bone density support
The Bottom Line on Maca Root for Women
Four clinical trials, a systematic review, and centuries of traditional use in the Peruvian Andes support maca root as a legitimate tool for women’s hormonal health — particularly for perimenopausal symptoms, libido, and energy.
The three things that determine whether it works for you: using gelatinized maca (not raw), using the right dose for your life stage (2–3.5g/day for hormonal goals), and giving it eight weeks of consistent daily use. Yellow maca covers most goals; add red maca if bone density is a specific concern.
Your next step: If you’re perimenopausal or dealing with low libido, start with 2g/day of gelatinized yellow maca with breakfast. Stack with ashwagandha in the evening if sleep or anxiety is also a concern. For more on building a complete women’s hormonal support protocol, see our guide to natural menopause relief.
⚕️ Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Maca root affects hormonal signaling — always consult your healthcare provider before starting it, especially if you have thyroid conditions, hormone-sensitive conditions, or take prescription medications including SSRIs or thyroid medications.
Written by Ethan Cole, Nutrition Expert | HerbzWay | Author Page
=== 🔗 OUTGOING LINKS FROM THIS ARTICLE ===
→ 🔗 Ashwagandha for Stress Relief: Dosage, Timing & What 12 Studies Show
→ 🔗 Natural 7 Herbs for Menopause Relief: That Actually Work
→ 🔗 Holy Basil Benefits (Tulsi): The Adaptogen You Haven’t Tried Yet