How to Lower Blood Sugar Naturally: 12 Proven Methods Ranked by Effect

Most “lower blood sugar naturally” lists treat a 30-minute walk, a cinnamon capsule, and six hours of quality sleep as if they’re interchangeable. They’re not. The clinical evidence behind each intervention differs by an order of magnitude — and spending your energy on the wrong methods while ignoring the most effective ones can mean months of effort with minimal results.
💡 Quick Answer: How to Lower Blood Sugar Naturally
The three highest-impact natural blood sugar interventions by clinical effect size are: (1) High-intensity interval training — HbA1c reduction of ~0.81% in meta-analysis; (2) Low-carbohydrate diet — HbA1c −0.29% to −2.0%; (3) Weight loss — approximately 0.1% HbA1c reduction per 1 kg lost. Berberine supplementation, time-restricted eating, and sleep optimization each contribute meaningful additive effects. Cinnamon and apple cider vinegar have real but small effects (< 0.2% HbA1c).
This guide ranks 12 proven methods by their HbA1c and fasting glucose effect sizes from published meta-analyses, so you can build your protocol around what the evidence actually supports.
📋 Written by Ethan Cole, Nutrition Expert | Meet Ethan →
- ✔ Verified against third-party Certificates of Analysis (COAs), current Amazon listings, and 2025–2026 clinical research
- 📅 Last Updated: May 2026
⚠️ This article does not constitute medical advice. If you manage blood sugar with prescription medication, discuss any supplement changes with your healthcare provider before making them.
⚠️This article contains affiliate links. If you purchase through our links, we may earn a small commission at no extra cost to you. See our Affiliate Disclosure for details.
Why Most “Natural” Blood Sugar Advice Misses the Point {#problem}
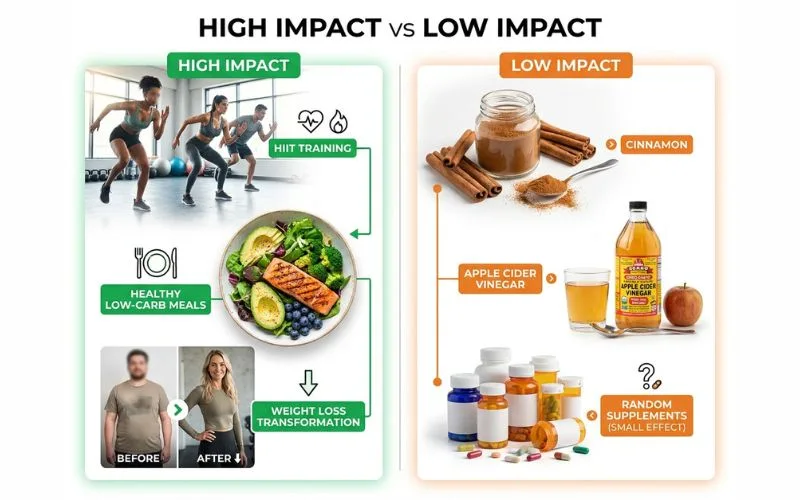
The problem with most blood sugar advice isn’t that it’s wrong — it’s that it treats all interventions as equally important. Lists of 15 tips imply that drinking more water is as impactful as doing HIIT three times a week. The research shows otherwise.
According to the American Diabetes Association’s 2024 Standards of Medical Care, lifestyle intervention remains the most powerful first-line tool for both prediabetes reversal and type 2 diabetes management. The ADA estimates that lifestyle changes alone can reduce the risk of progressing from prediabetes to type 2 diabetes by 58% over 3 years — more than any single medication.
But “lifestyle changes” isn’t a monolith. A 2024 network meta-analysis covering 158 studies and 17,059 participants found that high-intensity interval training (HIIT) reduced HbA1c significantly more than any other single exercise modality. A separate 2025 meta-analysis of intermittent fasting found a strong short-term HbA1c effect that largely disappeared after 3 months when fasting was discontinued. These are not minor distinctions — they should change how you prioritize your time.
What follows is an evidence-ranked guide. Each method includes the specific HbA1c or fasting glucose effect from the most rigorous available meta-analysis, so you can build a protocol that reflects the actual hierarchy of what works.
How to Read This List: Effect Size Explained {#how-to-read}
HbA1c is the primary metric used in most studies — it reflects your average blood sugar over the past 2–3 months. A reduction of 0.5% HbA1c is clinically meaningful. A 1.0% reduction is substantial. A 2.0% reduction is equivalent to adding a second diabetes medication.
Fasting plasma glucose (FPG) is your morning blood sugar before eating. Reductions of 5–15 mg/dL are clinically relevant for prediabetes management.
Effect sizes in this article come from published systematic reviews and meta-analyses — the highest level of evidence available for each intervention. Where studies measured different populations (prediabetes vs T2DM, different baseline HbA1c), effects are noted.
The Ranked Evidence Table: All 12 Methods {#ranked-table}
| Rank | Method | HbA1c Reduction | FPG Reduction | Evidence Level |
|---|---|---|---|---|
| 1 | HIIT Exercise | ~−0.81% | Significant | Strong (158 RCTs) |
| 2 | Low-Carb Diet | −0.29% to −2.0% | −7.12 mg/dL | Strong (21+ meta-analyses) |
| 3 | Weight Loss | ~−0.1% per kg lost | Proportional | Strong (multiple RCTs) |
| 4 | Berberine | −0.63% average | −0.82 mmol/L | Strong (37 RCTs) |
| 5 | Time-Restricted Eating | −0.11% to −0.75% short-term | −0.74 mmol/L | Moderate (8 RCTs) |
| 6 | Low-GI Diet | −0.5% (vs high-GI) | −127.7 vs 136.8 mg/dL | Moderate (18 RCTs) |
| 7 | Aerobic Exercise (150 min/week) | ~−0.56% | Significant | Strong (85 RCTs) |
| 8 | Sleep Optimization (7–9 hrs) | −0.2% to −0.5% | Significant | Moderate |
| 9 | Stress Reduction | −0.3% to −0.5% | Moderate | Moderate |
| 10 | Soluble Fiber Increase | ~−0.2% | −8 mg/dL | Moderate (multiple RCTs) |
| 11 | Apple Cider Vinegar | ~−0.1% (FPG −8 mg/dL) | −8 mg/dL | Low-Moderate (10 RCTs) |
| 12 | Cinnamon | −0.09% to −0.27% | Modest | Low-Moderate (10+ RCTs) |
Methods 1–4: High-Evidence Interventions {#tier1}
Method 1: High-Intensity Interval Training (HIIT)
Effect: ~−0.81% HbA1c | Strongest single exercise modality in head-to-head comparison

A landmark 2024–2025 network meta-analysis published in Diabetes Research and Clinical Practice (ScienceDirect, 2025) covered 158 randomized controlled trials with 17,059 participants testing different exercise types against each other. The finding: HIIT was associated with the greatest reduction in HbA1c of all types of exercise — outperforming aerobic exercise, resistance training, combined training, and physical activity advice.
HIIT works by rapidly depleting muscle glycogen stores during high-intensity bursts, which then draws circulating glucose into muscle cells for replenishment — producing an acute blood sugar-lowering effect that persists for hours. Repeated HIIT sessions also improve insulin receptor sensitivity over weeks.
What HIIT looks like practically:
- 20–30 minutes total workout time
- Alternating 20–40 second high-intensity bursts (sprint, cycling at max effort, jump squats) with 60–90 second recovery periods
- 2–3 sessions per week (the RCT data doesn’t show dose-response benefit beyond this frequency)
- No gym required — bodyweight HIIT at home produces equivalent glycemic outcomes
The key data point: A meta-analysis of aerobic exercise trials (Lancaster University, 2022) found that twelve-week or longer aerobic exercise programmes improve glycaemic control and BMI in adults with type 2 diabetes, with HbA1c reduction of approximately 0.56% — meaningful, but below HIIT’s effect size in the same network comparison.
Method 2: Low-Carbohydrate Diet
Effect: −0.29% to −2.0% HbA1c | −7.12 mg/dL FPG | Dose-dependent, best at 3 months

The mechanism is direct: fewer dietary carbohydrates means less glucose entering the bloodstream after eating, reducing both post-meal spikes and the baseline glycemic load the pancreas must manage.
A 2025 meta-analysis covering 27 RCTs with 2,870 participants found that LCDs improved glycemia short-term: HbA1c −0.29%, with the largest effect at 3 months. Fasting blood glucose decreased overall (−7.12 mg/dL).
The 0.29% figure represents a modest low-carbohydrate diet (< 130g carbs/day). More restrictive approaches — including very low-carb and ketogenic diets — show larger effects in some populations, with HbA1c reductions of up to 2.0% in people with elevated baseline values.
Practical approach:
- Reduce net carbohydrates to 50–130g/day as a starting range
- Prioritize protein and non-starchy vegetables as carb replacements
- Focus on eliminating the highest-glycemic sources first: refined grains, sugar-sweetened beverages, white rice, processed snack foods
- You don’t need ketosis to see blood sugar benefits — moderate carb reduction produces meaningful results
Important note: If you take insulin or sulfonylureas, reducing carbohydrate intake requires coordinated medication adjustment. Work with your doctor to prevent hypoglycemia when reducing carb intake.
Method 3: Weight Loss (5–10% of Body Weight)
Effect: ~0.1% HbA1c reduction per 1 kg lost | Diabetes remission possible at 10%+ loss

Body fat — particularly visceral fat around the abdomen and liver — directly drives insulin resistance. Fat cells in the liver and pancreas impair the insulin signaling pathway, and losing that fat reverses the impairment mechanically.
The DiRECT trial (Diabetes Remission Clinical Trial, UK), published in The Lancet, found that 46% of type 2 diabetic patients who lost ≥15 kg of body weight entered full diabetes remission — defined as HbA1c below 6.5% without medication — after one year. At 5-year follow-up, 13% maintained remission.
Even modest weight loss produces meaningful blood sugar improvement. The ADA estimates that each 1 kg of weight lost reduces HbA1c by approximately 0.1%, making a 10 kg loss roughly equivalent to adding a blood sugar medication.
Most effective weight loss approaches for blood sugar:
- Caloric restriction combined with low-carb eating produces the fastest initial glycemic improvement
- Time-restricted eating (see Method 5) supports weight loss and produces independent glycemic benefits
- Exercise + dietary change is significantly more effective for weight loss and blood sugar than either alone
Method 4: Berberine Supplementation
Effect: −0.63% HbA1c | −0.82 mmol/L FPG | Comparable to metformin in clinical trials

Berberine activates AMPK — the same pathway as metformin — and adds alpha-glucosidase inhibition and gut microbiome modulation as separate blood sugar-lowering mechanisms. A 2022 systematic review of 37 RCTs with 3,048 type 2 diabetes patients found significant reductions across all three primary blood sugar markers.
For the full clinical comparison between berberine and metformin, see our berberine vs metformin deep dive.
Practical protocol:
- 500 mg three times daily before meals (1,500 mg/day total)
- Take 20–30 minutes before your largest carbohydrate meals
- Give it 12 weeks minimum before evaluating HbA1c effect
- Tell your doctor you’re using it — drug interactions exist, particularly with statins and blood thinners
Methods 5–8: Moderate-Evidence Interventions {#tier2}
Method 5: Time-Restricted Eating (TRE)
Effect: −0.11% HbA1c short-term | −0.74 mmol/L FPG | Effects attenuate after 3 months if discontinued
Time-restricted eating — confining all food intake to a 6–10 hour window each day — improves blood sugar through two mechanisms: it aligns insulin secretion with circadian biology (which optimizes insulin sensitivity), and it reduces the total number of hours the pancreas must produce insulin responses.
A 2025 meta-analysis of TRE in type 2 diabetes found that TRE significantly reduced fasting glucose (mean difference: −0.74 mmol/L) and glycated hemoglobin (ΔHbA1c: −0.11%) and increased time in range (TIR) for blood glucose (+10.51%).
The +10.51% improvement in time-in-range is particularly relevant for continuous glucose monitor (CGM) users — it means a meaningful reduction in the hours per day spent above target glucose levels.
Important caveat: A separate 2025 meta-analysis found that IF decreased HbA1c significantly compared to control diets short-term (< 3 months) but benefits did not persist after discontinuation. TRE is most effective as an ongoing practice, not a short course.
Practical implementation:
- Common protocol: 16:8 (16-hour fast, 8-hour eating window)
- Eating window: 10 a.m. to 6 p.m. or 12 p.m. to 8 p.m.
- Morning coffee (black) is generally acceptable without breaking the fast for blood sugar purposes
- If on diabetes medication, work with your doctor — fasting periods increase hypoglycemia risk
Method 6: Low-Glycemic Index Diet
Effect: −0.5% HbA1c vs high-GI diet | Sustained effect with continued adherence
The glycemic index (GI) measures how quickly a carbohydrate food raises blood sugar compared to pure glucose. Low-GI foods (under 55) produce gradual glucose rises; high-GI foods (above 70) produce rapid spikes. Swapping high-GI for low-GI foods, without necessarily reducing total carbohydrate intake, produces meaningful blood sugar improvement.
A meta-analysis of 18 RCTs found that low-GI diets reduced HbA1c by approximately 0.5% compared to higher-GI diets in people with diabetes, alongside improvements in total cholesterol and LDL.
Highest-impact swaps:
| Instead of (High GI) | Choose (Low GI) | GI Difference |
|---|---|---|
| White rice (GI ~73) | Basmati rice or quinoa (GI 50–53) | −20–23 pts |
| White bread (GI ~75) | Sourdough or 100% rye (GI 48–54) | −21–27 pts |
| Instant oatmeal (GI ~79) | Steel-cut oats (GI ~42) | −37 pts |
| Russet potato (GI ~85) | Sweet potato (GI ~54) | −31 pts |
| Cornflakes (GI ~93) | All-Bran or bran flakes (GI 42–55) | −38–51 pts |
The most practical low-GI approach: add protein or fat to any carbohydrate meal, which lowers the GI of the whole meal by slowing gastric emptying. A baked potato with chicken and olive oil has a significantly lower effective GI than the potato eaten alone.
Method 7: Standard Aerobic Exercise (150 min/week)
Effect: ~−0.56% HbA1c | Consistent across all fitness levels and age groups
While HIIT produces the largest blood sugar effect per unit of time, standard aerobic exercise — walking, cycling, swimming, dancing — at 150 minutes per week remains one of the most robustly proven blood sugar interventions in the literature. A meta-analysis of 85 RCTs with 5,535 participants confirmed significant HbA1c reduction with regular aerobic exercise.
The mechanism: aerobic exercise increases GLUT4 transporter activity in skeletal muscle — the protein that moves glucose from the bloodstream into cells. This effect is partly insulin-independent, meaning it works even when insulin signaling is impaired.
For people starting from zero:
- Start with 10-minute post-meal walks — post-meal exercise specifically targets the postprandial glucose spike and can reduce it by 20–30%
- Build to 30 minutes of brisk walking five times per week
- Any movement is better than none; consistency over intensity is the right initial priority
- Resistance training adds separate blood sugar benefits through increased muscle mass (more metabolically active tissue for glucose uptake)
Method 8: Sleep Optimization
Effect: −0.2% to −0.5% HbA1c | Foundational for all other interventions

This is the most underrated item on every blood sugar list. Poor sleep — defined as consistently under 6 hours — raises cortisol and growth hormone levels that directly counteract insulin’s glucose-lowering action. One night of poor sleep can reduce insulin sensitivity by 20–25% the following day.
A meta-analysis published in Diabetes Care found that each additional hour of sleep beyond 5 hours per night was associated with a 0.2% reduction in HbA1c in diabetic populations, up to the 7–9 hour optimal range.
Practical sleep protocol for blood sugar management:
- Target 7–9 hours per night consistently (weekend catch-up sleep doesn’t undo weekday deficits)
- Avoid screens 60 minutes before bed — blue light suppresses melatonin, delaying sleep onset
- Keep your bedroom below 68°F — cooler temperatures improve sleep depth and duration
- Avoid alcohol within 3 hours of bedtime — it disrupts REM sleep and raises morning blood sugar
- Exercise timing: morning or afternoon exercise improves sleep quality; intense exercise within 2 hours of bedtime may delay sleep onset
Methods 9–12: Low-to-Moderate Effect Interventions {#tier3}
Method 9: Stress Reduction (Cortisol Management)
Effect: −0.3% to −0.5% HbA1c with consistent stress management practices
Chronic psychological stress raises cortisol, which directly stimulates hepatic glucose production and reduces insulin sensitivity. This is why many people with well-managed diets still see elevated fasting blood sugar during high-stress periods.
Mindfulness-based stress reduction (MBSR) has 8-week RCT data showing meaningful HbA1c reduction. Yoga intervention trials show comparable results. The specific stress-reduction activity matters less than its consistency — daily practice of any effective method produces gradual but meaningful cortisol normalization.
For the ashwagandha cortisol connection, see our ashwagandha for stress relief guide — reducing chronic cortisol elevation directly supports blood sugar management.
Method 10: Soluble Fiber Increase
Effect: ~−0.2% HbA1c | −8 mg/dL FPG from multiple RCTs
Soluble fiber — found in oats, legumes, psyllium husk, chia seeds, and flaxseed — dissolves in water to form a gel that slows gastric emptying and blunts post-meal glucose absorption. It also feeds beneficial gut bacteria, supporting microbiome-mediated insulin sensitivity.
Psyllium husk at 10–15g/day before main meals has the most direct blood sugar evidence among fiber supplements. Oat beta-glucan at 3–6g/day also shows consistent post-meal glucose blunting in RCTs.
Adding these to your existing diet — rather than removing foods — is the lowest-friction blood sugar intervention available.
Method 11: Apple Cider Vinegar
Effect: ~−8 mg/dL FPG | Small but consistent signal across 10 RCTs

Apple cider vinegar (ACV) taken before high-carbohydrate meals reduces post-meal glucose spikes through acetic acid’s alpha-glucosidase inhibition — the same mechanism as berberine and acarbose, but at a fraction of the effect size. A 2021 analysis found that people with type 2 diabetes who had apple cider vinegar lowered their fasting blood glucose by about 8 milligrams per deciliter.
This is a real effect. It is small. ACV should be viewed as a useful add-on, not a primary intervention.
If you use it: 1–2 tablespoons diluted in water, taken 20–30 minutes before your largest carbohydrate meal. Never drink it undiluted — the acidity damages tooth enamel and the esophagus. Avoid if you have gastroparesis (slow stomach emptying) — it worsens the condition.
Method 12: Cinnamon
Effect: −0.09% to −0.27% HbA1c | Inconsistent across studies
Cinnamon contains compounds that may improve insulin sensitivity and inhibit digestive enzymes that break down carbohydrates. The meta-analysis data shows a small but real effect — most consistently on fasting glucose rather than HbA1c. The effect is inconsistent across populations and dose-dependent.
Ceylon cinnamon (true cinnamon) is preferred over Cassia cinnamon for regular use — Cassia contains coumarin at levels that may affect liver function at high doses. 1–3g/day of Ceylon cinnamon with meals is the range studied in positive trials.
Cinnamon belongs in your blood sugar toolkit. It should not be the centerpiece of it.
What Won’t Move the Needle Much (But Gets Oversold) {#wont-work}
Drinking More Water
Hydration prevents hemoconcentration (elevated blood glucose from reduced blood volume), and dehydration can transiently raise readings. But in a person who is reasonably hydrated, drinking more water produces no direct blood sugar reduction. This is consistently listed in “15 ways to lower blood sugar” articles — it doesn’t belong at the same level as diet, exercise, or berberine.
Most Supplement Powders and “Blood Sugar Support” Blends
Products combining small doses of berberine, cinnamon, chromium, gymnema, and bitter melon in a “proprietary blend” typically contain none of the individual ingredients at doses proven to produce effects. Each component in a comprehensive formula is usually far below the therapeutic threshold. Stick to single-ingredient supplements at studied doses.
Chromium
Often marketed aggressively for blood sugar. The evidence is modest — a meta-analysis showed small improvements in insulin sensitivity in insulin-resistant individuals but no consistent HbA1c reduction. Not worth prioritizing over the top-tier methods.
Bitter Melon (Momordica charantia)
Traditional use is long-standing; clinical trial evidence is inconsistent. Multiple RCTs show no significant benefit over placebo; a few show modest fasting glucose reduction. Evidence is insufficient to recommend it as a reliable blood sugar intervention.
Your 30-Day Priority Protocol {#protocol}
Based on the effect sizes above, here’s the rational starting order for someone newly diagnosed with prediabetes or early T2DM:
Week 1–2: Establish the Baseline
- Start tracking fasting blood glucose every morning (basic glucometer, ~$20)
- Reduce the highest-GI foods: cut sugar-sweetened beverages entirely, reduce white rice/bread/processed snacks
- Add 10-minute post-meal walks after your two largest meals
- Start berberine HCl 500 mg before each main meal
Week 3–4: Add the High-Impact Layer
- Replace 2 of your aerobic cardio sessions with a 20-minute HIIT protocol
- Shift eating to a 10:00 a.m.–7:00 p.m. window (if medically appropriate)
- Add a source of soluble fiber before your largest carbohydrate meal (1 tbsp psyllium husk in water)
- Prioritize sleep — set a consistent bedtime 30 minutes earlier than current
Month 2+: Build and Refine
- Assess fasting glucose trends from your 30-day log
- HbA1c recheck at 3 months — your doctor can order this
- Adjust carbohydrate intake based on glucose response (use your glucometer 2 hours after meals to identify your personal high-response foods)
- Add ashwagandha if stress and cortisol elevation is a documented concern
What to expect realistically: At the top of the evidence hierarchy, consistent HIIT + low-carb diet + berberine + 7+ hours of sleep, sustained for 12 weeks, could plausibly produce a combined HbA1c reduction of 1.5–2.5% — enough to move from prediabetes to normal range, or from early T2DM to well-controlled. This is not a replacement for medical care. It’s a complement to it.
⚠️ Medical Disclaimer: This article is for informational purposes only. The protocols described above are general wellness approaches, not medical prescriptions. If you have diabetes or prediabetes, work with your healthcare provider before making significant dietary, exercise, or supplementation changes.
FAQ: How to Lower Blood Sugar Naturally {#faq}
What is the fastest way to lower blood sugar naturally?
For an immediate reduction in an already-elevated blood sugar reading, physical activity — even a 15–20 minute brisk walk — is the fastest natural intervention. Exercise acutely drives glucose into muscle cells independent of insulin. For sustained reduction over days and weeks, the combination of HIIT exercise + low-carb diet produces the fastest evidence-based HbA1c improvement, with measurable changes beginning at 3–4 weeks.
What foods lower blood sugar quickly?
No food “lowers” blood sugar — foods either raise it quickly (high GI) or slowly (low GI). The fastest way to address an elevated blood sugar through food is to stop adding glucose to the bloodstream: skip the next carbohydrate meal or replace it with protein and non-starchy vegetables. Foods rich in soluble fiber (chia seeds, legumes, oats) slow glucose absorption from subsequent meals. Vinegar (ACV) taken before a high-carb meal reduces the post-meal glucose spike by slowing carbohydrate digestion.
How much can diet alone lower HbA1c?
A low-carbohydrate diet alone can reduce HbA1c by 0.29–2.0% depending on baseline values and adherence level. The effect is largest in people with higher starting HbA1c. A strict very-low-carb approach in someone with T2DM starting at 8.5% HbA1c has potential for 1.5–2.0% reduction over 3 months. For people with prediabetes (HbA1c 5.7–6.4%), the effect is smaller (0.3–0.5%) but still meaningful for reversal purposes.
Does exercise lower blood sugar immediately?
Yes — both immediately and over time. A single aerobic exercise session can lower blood glucose by 10–30 mg/dL during and for up to 24 hours after activity, depending on intensity and duration. HIIT has a more pronounced immediate effect than low-intensity walking. Regular exercise also produces long-term insulin sensitivity improvements through increased GLUT4 transporter expression in skeletal muscle — this is an adaptation that takes 2–4 weeks of consistent training to fully develop.
Can you lower HbA1c in 2 weeks?
Fasting blood glucose can improve meaningfully within 1–2 weeks of dietary changes. HbA1c reflects a 2–3 month average — you cannot meaningfully move an HbA1c reading in 2 weeks regardless of intervention. The standard assessment window for lifestyle interventions is 12 weeks (one full HbA1c cycle). Expect fasting glucose to respond first, followed by post-meal glucose patterns, followed by HbA1c at the 3-month recheck.
Is berberine effective for naturally lowering blood sugar?
Yes — berberine has one of the strongest natural blood sugar evidence bases available, with a 2022 meta-analysis of 37 RCTs (3,048 patients) showing HbA1c reduction of −0.63% and FPG reduction of −0.82 mmol/L, both statistically significant. It activates AMPK (the same pathway as metformin) and adds alpha-glucosidase inhibition. For the full comparison, see our berberine vs metformin guide.
What naturally lowers blood sugar overnight?
Fasting blood glucose (morning reading) is largely determined by the liver’s overnight glucose production rate, which is governed by cortisol and glucagon. The most effective overnight interventions are: (1) low-carb dinner — reduces liver glycogen repletion that drives overnight glucose release; (2) sleep quality and duration — 7–9 hours reduces cortisol-mediated overnight gluconeogenesis; (3) avoiding late-night eating — a 12-hour fast ending at breakfast improves morning glucose sensitivity; (4) evening exercise reduces glycogen stores that are then refilled from blood glucose overnight.
Does cinnamon really lower blood sugar?
Yes, modestly. Meta-analyses show cinnamon reduces fasting blood glucose and has a small HbA1c effect (−0.09% to −0.27%) in people with prediabetes and T2DM. The effect is real but smaller than dietary, exercise, or berberine interventions. Use Ceylon cinnamon (not Cassia) for regular use to avoid coumarin accumulation. Consider it a useful supplement to the core interventions, not a primary strategy.
How much does losing weight reduce blood sugar?
Approximately 0.1% HbA1c reduction per 1 kg of weight lost in people with type 2 diabetes. More importantly, the DiRECT trial showed that weight loss of ≥15 kg produced full diabetes remission (HbA1c < 6.5% without medication) in 46% of participants at one year. Even 5–10% of body weight loss consistently improves HbA1c by 0.5–1.0% and significantly reduces insulin resistance. Weight loss is among the most powerful tools for prediabetes reversal specifically.
Is intermittent fasting good for blood sugar?
Intermittent fasting produces consistent short-term blood sugar improvements — HbA1c reduction of approximately 0.11–0.75% and significant fasting glucose reduction. The key limitation is sustainability: a 2025 meta-analysis found that the metabolic benefits largely disappear after stopping IF. This makes it most effective as an ongoing lifestyle practice rather than a short course. Time-restricted eating (16:8 or 14:10 window) is the most practically sustainable IF protocol for blood sugar management.
The Bottom Line {#conclusion}
The 12 methods in this guide are all supported by clinical evidence — but they’re not equal. HIIT, low-carb diet, weight loss, and berberine sit in a different tier than cinnamon and ACV, and treating them as equivalent leads to misplaced effort.
The most effective natural approach combines the top-tier interventions simultaneously: consistent HIIT 2–3 times per week, meaningful carbohydrate reduction, sleep optimization, and berberine before meals. Each works through a different mechanism — together, their effects are additive. People who implement all four consistently for 12 weeks can expect HbA1c reductions that rival prescription medication.
Work with your doctor. Monitor your numbers. Invest your effort in the interventions the evidence actually supports.
This article is for informational purposes only and does not constitute medical advice.
Written by Ethan Cole, Nutrition Expert | Meet Ethan →
=== 🔗 OUTGOING LINKS FROM THIS ARTICLE ===
→ 🔗 Is Berberine Better Than Metformin? A Natural Alternative Deep Dive
→ 🔗 Ashwagandha for Stress Relief: Dosage, Timing & What 12 Studies Show