Is Berberine Better Than Metformin? A Natural Alternative Deep Dive
Thirty-eight million Americans have type 2 diabetes, and another 96 million have prediabetes. Metformin has been their first-line pharmaceutical option for over 60 years. Berberine — a plant-derived compound found in barberry, goldenseal, and Oregon grape — has been prescribed in Chinese medicine for blood sugar management for centuries. A landmark 2012 meta-analysis found its HbA1c reduction was statistically equivalent to metformin. That comparison triggered a wave of interest that hasn’t slowed down.
💡 Quick Answer: Is Berberine Better Than Metformin?
Berberine and metformin activate the same primary mechanism (AMPK) and produce comparable HbA1c reductions in clinical trials — approximately 0.7–2.0% depending on baseline. Berberine is not a drug, has no prescription requirement, and showed fewer GI side effects than metformin in a 2025 head-to-head RCT. However, berberine cannot replace metformin for everyone — it lacks long-term safety data, cardiovascular outcome evidence, and physician monitoring. The most supported use case is either: berberine for prediabetes/early T2DM with physician awareness, or berberine as an add-on to metformin for enhanced blood sugar control.
This article covers the clinical comparison data honestly, explains where berberine falls short, identifies who can reasonably consider it, and presents the growing evidence for using both together.
📋 Written by Ethan Cole, Nutrition Expert | Meet Ethan →
- ✔ Verified against third-party Certificates of Analysis (COAs), current Amazon listings, and 2025–2026 clinical research
- 📅 Last Updated: May 2026
⚠️ This article does not constitute medical advice. If you manage blood sugar with prescription medication, discuss any supplement changes with your healthcare provider before making them.
⚠️This article contains affiliate links. If you purchase through our links, we may earn a small commission at no extra cost to you. See our Affiliate Disclosure for details.
The Scale of the Problem: Why This Question Matters {#scale}
The numbers make this question urgent rather than academic. According to the Centers for Disease Control and Prevention, more than 38 million Americans have diabetes, approximately 90–95% of which is type 2, and an estimated 96 million adults have prediabetes. Metformin is the most prescribed diabetes medication in the United States — approximately 90 million prescriptions annually — and has been first-line therapy for type 2 diabetes in American clinical guidelines since 1995.
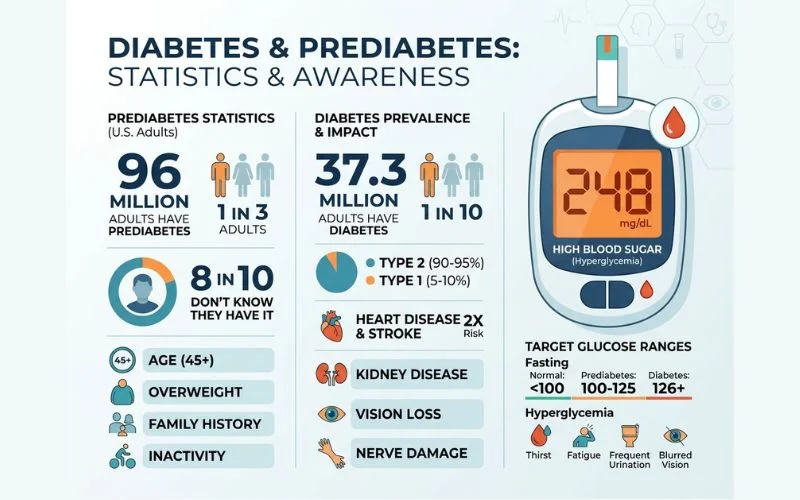
Its side effect profile is the reason people go looking for alternatives. Up to 30% of people prescribed metformin experience significant gastrointestinal side effects — nausea, diarrhea, stomach cramping — and approximately 5–10% discontinue it for this reason. Metformin also causes vitamin B12 depletion in roughly 30% of long-term users, requiring monitoring or supplementation.
Berberine’s appeal is structural: it’s accessible without a prescription, has a growing clinical trial base, and activates the same primary metabolic pathway. Understanding the data honestly — including its gaps — is the starting point for any reasonable decision.
How Berberine and Metformin Both Work {#mechanism}
The shared mechanism is the most important piece of this comparison.
The AMPK Pathway
Both berberine and metformin activate AMP-activated protein kinase (AMPK) — an enzyme that functions as a cellular energy sensor and master metabolic switch. When AMPK is activated, it produces three blood sugar-relevant effects:
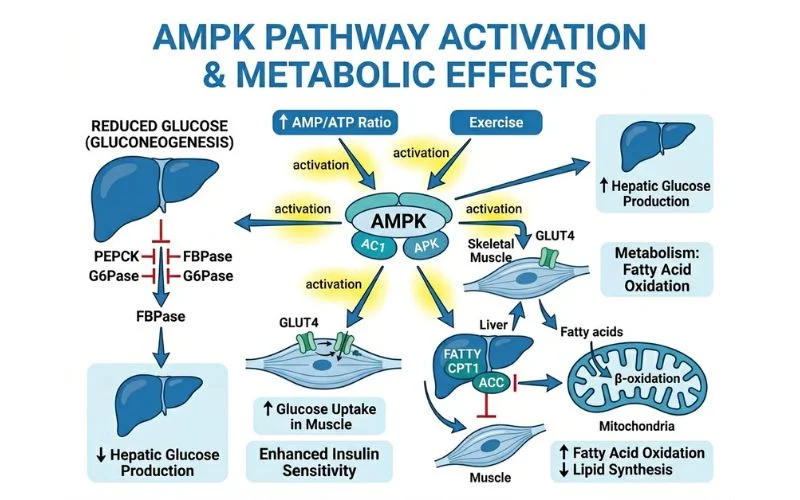
- Reduces hepatic glucose production — suppresses the liver’s gluconeogenesis (the process of generating glucose from non-carbohydrate sources), which is a major driver of fasting blood glucose elevation in T2DM
- Improves insulin sensitivity in skeletal muscle — enhances glucose uptake into muscle cells, reducing circulating blood glucose
- Reduces fat accumulation — AMPK activation inhibits fatty acid synthesis and promotes fat oxidation, supporting weight-related metabolic improvement
This is why both compounds produce overlapping outcomes in clinical trials: they’re working on the same cellular lever.
Where Their Mechanisms Diverge
Berberine has two additional mechanisms metformin lacks:
Alpha-glucosidase inhibition: Berberine inhibits the enzyme that breaks down dietary carbohydrates in the gut — the same mechanism as the diabetes drug acarbose. This slows post-meal glucose absorption, blunting blood sugar spikes after eating. This is why berberine often shows stronger post-prandial glucose reduction than metformin in direct comparisons.
Gut microbiome modulation: Berberine significantly alters gut microbiota composition — increasing Akkermansia muciniphila and Bacteroides fragilis populations, which are associated with improved insulin sensitivity and reduced metabolic inflammation. A 2024 PMC review (PMC10968539) identified this gut-mediated mechanism as a distinct pathway that may explain why some individuals respond to berberine even when AMPK-targeting drugs have limited effect.
Metformin also affects the gut microbiome, but through different bacterial populations. The overlap creates a genuine mechanistic rationale for using both together.
Head-to-Head Clinical Data: What the Trials Show {#trials}
The 2012 Meta-Analysis (The Headline Number)
The study most frequently cited is a 2012 meta-analysis by Dong et al. (Evidence-Based Complementary and Alternative Medicine, PMC3478874) covering 14 randomized trials with 1,068 participants. The finding: compared with oral hypoglycemic drugs including metformin, berberine did not demonstrate significantly different glycemic control — meaning the two were statistically equivalent for HbA1c and fasting glucose reduction.
Berberine achieved comparable HbA1c reductions to metformin, glipizide, and rosiglitazone in direct comparison arms.
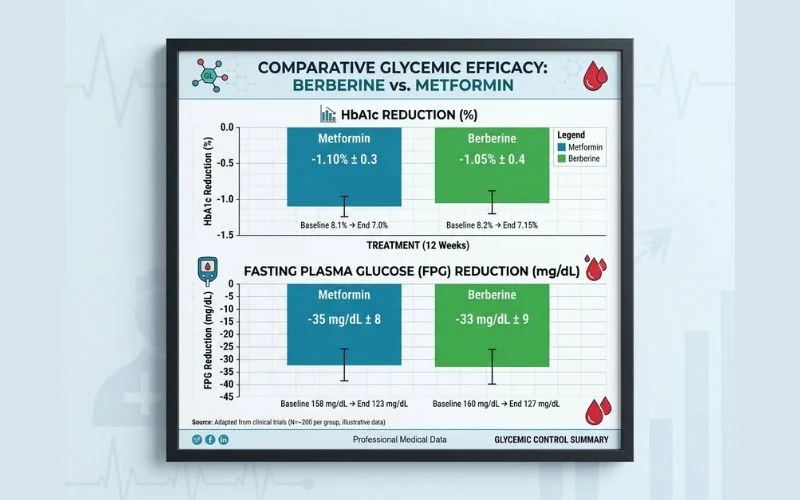
The 2025 Prediabetes Head-to-Head RCT (The Most Recent Data)
A 2025 randomized clinical trial (Chaudhary et al., International Journal of Basic & Clinical Pharmacology, IJBCP) enrolled 90 prediabetic participants in a direct head-to-head comparison:
- Berberine HCl: 500 mg twice daily (1,000 mg/day total)
- Metformin: 500 mg twice daily (1,000 mg/day total)
- Duration: 12 weeks
| Outcome | Berberine Group | Metformin Group | Significance |
|---|---|---|---|
| FPG reduction | 109.8 → 97.2 mg/dL (−12.6 mg/dL) | 110.2 → 99.4 mg/dL (−10.8 mg/dL) | Berberine numerically superior |
| PPG reduction | 156.4 → 134.6 mg/dL (−21.8 mg/dL) | 157.1 → 137.8 mg/dL (−19.3 mg/dL) | Berberine numerically superior |
| HbA1c reduction | −0.31% | −0.28% | P=0.04 (berberine significantly better) |
| GI adverse events | 20% | 30% | Berberine better tolerated |
The 2025 data shows berberine achieving slightly better blood sugar outcomes with fewer GI side effects than metformin — in a prediabetes population at the same milligram dose.
The 2022 PMC Meta-Analysis (37 Studies, 3,048 Patients)
A 2022 systematic review and meta-analysis (PMC9709280) covering 37 randomized controlled trials with 3,048 type 2 diabetes patients found:
| Metric | Berberine Effect | Statistical Significance |
|---|---|---|
| Fasting plasma glucose (FPG) | −0.82 mmol/L | P < 0.001 |
| HbA1c | −0.63% | P < 0.001 |
| 2-hour postprandial glucose (2hPBG) | −1.16 mmol/L | P < 0.001 |
All three primary blood sugar markers improved significantly with berberine. No serious adverse events attributed to berberine were reported across the 37 trials.
What This Data Confirms — and Doesn’t
The clinical evidence for berberine as a blood sugar-lowering intervention is genuine and consistent. Multiple meta-analyses across thousands of patients confirm significant, meaningful HbA1c reduction. The head-to-head comparison with metformin shows comparable or slightly superior glycemic outcomes at equivalent doses in prediabetes.
What this data cannot tell you: long-term cardiovascular outcomes, 10-year safety data, or whether berberine prevents diabetes complications as effectively as metformin. Metformin has this data — decades of it. Berberine does not.
Where Berberine Falls Short Compared to Metformin {#limitations}
This section is the most important one for anyone seriously considering a switch — and the one most articles handle poorly.
Gap 1: No Cardiovascular Outcome Data
Metformin’s position as the first-line diabetes medication rests not just on blood sugar reduction but on its demonstrated cardiovascular benefits. The UKPDS trial (UK Prospective Diabetes Study) found that intensive blood glucose management with metformin reduced cardiovascular events — heart attacks, strokes — and diabetes-related deaths.
Berberine has promising cardiovascular preclinical data (reduces LDL, triglycerides, blood pressure in trials) but has not been tested in a long-term outcome trial that measures whether it reduces cardiovascular events or mortality in diabetic patients. For someone with established cardiovascular disease or high cardiovascular risk, this gap is clinically significant.
Gap 2: Long-Term Safety Data
Metformin has been used daily in millions of patients for over 60 years. Its safety profile at therapeutic doses is well-characterized: B12 depletion with long-term use, lactic acidosis risk at very high doses in specific conditions (rare), and kidney function monitoring requirements. These are known, manageable risks.
Berberine’s longest clinical trials run approximately 6 months. There is no 5-year or 10-year safety dataset in diabetic populations. This doesn’t mean it’s unsafe — the 37-trial meta-analysis reported no serious adverse events — but the uncertainty is real.
Gap 3: Low Bioavailability (The Math Problem)
Standard berberine hydrochloride (HCl) has poor oral bioavailability — a significant fraction is not absorbed from the gut into the bloodstream. This explains why clinical trials require 1,000–1,500 mg/day (divided doses) compared to metformin at 500–2,000 mg/day.
The clinical trials showing equivalent outcomes did use high doses of standard berberine HCl. But it means the comparison is not “equal doses” — and that GI side effects from berberine partly occur because a large amount remains in the gut rather than being absorbed.
Newer formulations (berberine phytosome) achieve approximately 5x higher bioavailability, allowing effective use at lower total doses. These are legitimate improvements but have less clinical trial data than standard HCl formulations.
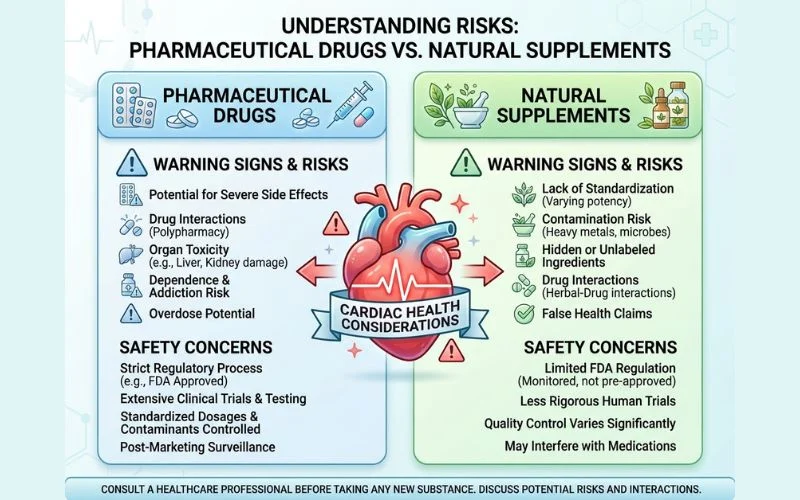
Gap 4: No Regulatory Oversight
Metformin is a regulated pharmaceutical. Every batch is tested for potency and purity. Prescriptions require physician oversight, with kidney function monitoring and regular HbA1c checks built into standard care.
Berberine is a dietary supplement in the United States. It is not FDA-approved for blood sugar management. Supplement manufacturing standards (GMP) are less stringent than pharmaceutical standards, and product quality varies significantly between brands. Someone using berberine without physician oversight will not automatically receive the monitoring that accompanies metformin prescriptions.
Gap 5: Drug Interactions
Berberine inhibits several CYP450 liver enzymes — particularly CYP3A4 and CYP2D6 — which metabolize a wide range of prescription medications. This creates the potential for meaningful drug interactions with:
- Statins (increased statin blood levels → higher rhabdomyolysis risk)
- Blood thinners (warfarin, clopidogrel)
- Antihypertensives
- Cyclosporine and other immunosuppressants
- Some antidepressants
Anyone taking multiple prescription medications must discuss berberine with their doctor before starting.
Who Can Reasonably Consider Berberine {#who-can}
With those limitations clearly stated, here are the populations for whom berberine has a reasonable evidence base:

Prediabetes (Strongest Case)
The 2025 head-to-head RCT used a prediabetes population specifically. For adults with prediabetes who are not yet on metformin and whose physician has recommended lifestyle-first management, berberine at 1,000–1,500 mg/day represents a clinically supported natural option. The key: discuss it with your doctor, monitor your blood sugar numbers, and don’t use it as an excuse to avoid lifestyle changes that remain the most effective prediabetes intervention.
Early Type 2 Diabetes (Physician-Supervised)
For newly diagnosed T2DM patients who are trying to delay or avoid metformin initiation while maximizing lifestyle intervention, berberine has comparable short-term blood sugar data. This is a physician conversation, not a self-management decision. Monitoring matters.
Metformin-Intolerant Patients
For people who cannot tolerate metformin’s GI side effects and whose physicians are exploring alternatives, berberine represents a legitimate consideration given equivalent blood sugar outcomes and fewer GI adverse events in the 2025 RCT. This requires medical supervision.
As a Complement to Existing Treatment
The strongest practical case for berberine may not be “instead of” but “alongside” — see the next section.
Can You Take Berberine and Metformin Together? {#combination}
This is the most underreported aspect of the berberine research — and it changes the practical calculus significantly.
A 2021 Italian randomized controlled trial (PMC8308828) tested berberine + hesperidin + chromium picolinate as an add-on to existing metformin therapy in type 2 diabetes patients with suboptimal glycemic control. After 12 weeks:
- HbA1c decreased 7.5% in the metformin + berberine group vs. no change in metformin-only group (P<0.01)
- Fasting blood glucose dropped from 145 to 128 mg/dL (−11.7%) in the combination group vs. no significant change in control (P<0.05)
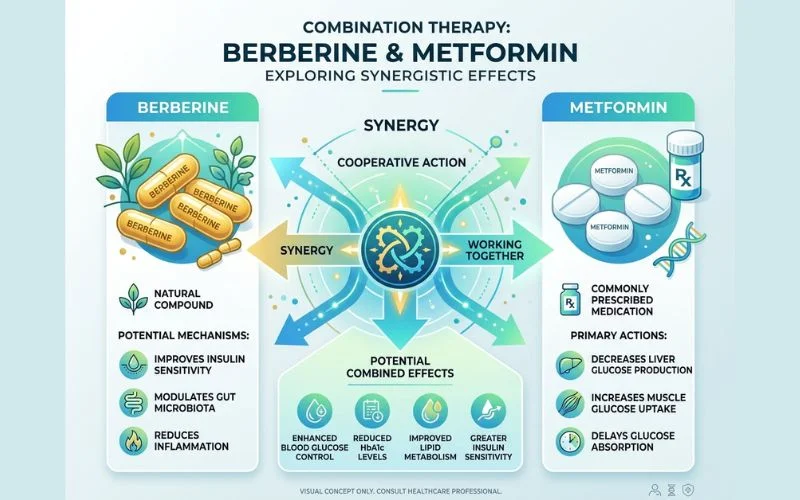
Because berberine and metformin activate AMPK through different molecular initiators and berberine adds alpha-glucosidase inhibition as a separate mechanism, combining them produces additive blood sugar-lowering effects — not just duplication.
The clinical implication: for someone already on metformin who wants better blood sugar control without adding another prescription medication, adding berberine as an adjunct has clinical support. This also allows metformin dose reduction in some cases, which may reduce GI side effects.
Critical note: Adding berberine to metformin increases hypoglycemia risk. Monitor blood sugar carefully, inform your doctor, and adjust dosing accordingly. This is not a self-managed addition.
Berberine Forms and the Bioavailability Problem {#forms}
If you’re going to use berberine, the form you choose affects how much actually reaches your bloodstream — and therefore how effective your dose is.
| Form | Bioavailability | Effective Daily Dose | Cost | Best For |
|---|---|---|---|---|
| Berberine HCl (standard) | ~5% oral absorption | 1,000–1,500 mg/day | $ | Most clinical trial evidence; widely available |
| Berberine Phytosome | ~5× higher than HCl | 500–600 mg/day | $$$ | Lower dose for similar effect; fewer GI side effects |
| Berberine fumarate/succinate | Higher than HCl | 800–1,000 mg/day | $$ | Better absorption than HCl; less available |
| Berberine with black pepper (BioPerine) | Modestly enhanced | 1,000–1,200 mg/day | $$ | Budget improvement over standard HCl |
The practical takeaway:
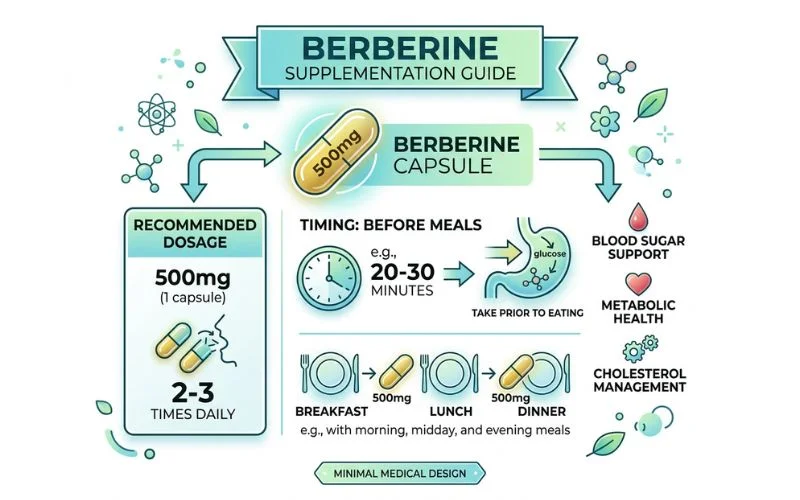
Berberine HCl at 500 mg three times daily (1,500 mg/day total, taken before meals) is the protocol used in most positive clinical trials and remains the most evidence-backed approach. Phytosome forms are legitimate improvements for absorption but have less direct clinical trial data for blood sugar outcomes specifically.
If GI tolerance is your main concern, phytosome berberine at 500–600 mg/day may deliver comparable blood sugar effects with significantly less GI discomfort than 1,500 mg/day of HCl.
Timing matters: Take berberine 20–30 minutes before meals. The alpha-glucosidase inhibition mechanism works at the gut level to blunt post-meal glucose spikes — this requires the compound to be present when carbohydrates arrive. Taking berberine between meals or at bedtime misses this mechanism.
Berberine Dosage for Blood Sugar {#dosage}
Based on clinical trial data:
| Population | Dose | Form | Timing |
|---|---|---|---|
| Prediabetes | 500 mg 2–3x/day (1,000–1,500 mg total) | HCl or phytosome | Before each main meal |
| Type 2 Diabetes (monotherapy) | 500 mg 3x/day (1,500 mg total) | HCl | Before 3 meals |
| Add-on to Metformin | 500 mg 2x/day (start low) | HCl or phytosome | Before 2 main meals |
| Phytosome form | 500 mg 1–2x/day | Phytosome | Before main meals |
Minimum trial period: 8–12 weeks before evaluating effectiveness. HbA1c changes require 3 months to fully reflect in lab results — short-term testing only shows fasting glucose trends.
Monitor while using berberine: Fasting blood glucose at home (if you have a glucometer), and HbA1c via your doctor every 3 months initially. Berberine lowers blood sugar — if you’re also on medication, hypoglycemia is a real risk that requires monitoring.
Side Effects and Safety Comparison {#safety}
| Factor | Berberine | Metformin |
|---|---|---|
| GI side effects | Mild — 20% (2025 RCT) | Moderate — 30% (2025 RCT); up to 30–40% in broader literature |
| Hypoglycemia risk | Low (glucose-dependent mechanism) | Low at standard doses |
| B12 depletion | Not documented | Yes — in ~30% of long-term users |
| Kidney contraindication | Caution with CKD | Contraindicated with significant CKD |
| Liver safety | Rare cases reported at high dose | Rare lactic acidosis in specific conditions |
| Drug interactions | Significant (CYP3A4/2D6) | Fewer interactions overall |
| Long-term safety data | Limited (< 1 year trials) | Decades of data |
| Prescription required | No | Yes |
| FDA regulated | No (dietary supplement) | Yes (pharmaceutical) |
| Cardiovascular outcomes data | None | Yes (UKPDS trial) |
→ 🔗 NIH — Berberine consumer information – FDA regulatory status and safety overview
⚠️ Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Berberine is not FDA-approved for diabetes or prediabetes management. If you have diabetes or prediabetes, work with your healthcare provider before making any changes to your treatment plan.
FAQ: Is Berberine Better Than Metformin? {#faq}
Is berberine as effective as metformin for blood sugar?
In clinical trials, yes — berberine produces comparable HbA1c and fasting glucose reductions to metformin. A 2012 meta-analysis of 14 RCTs (1,068 patients) found no statistically significant difference in glycemic control between berberine and metformin. A 2025 head-to-head RCT in prediabetes found berberine slightly outperformed metformin on FPG, PPG, and HbA1c at equivalent doses, with fewer GI side effects. For short-term blood sugar outcomes, the evidence supports equivalence or near-equivalence.
Can berberine replace metformin?
For some people in specific situations, berberine may be a reasonable alternative — particularly for prediabetes, early type 2 diabetes in otherwise healthy adults, or metformin-intolerant patients. However, berberine cannot replace metformin’s cardiovascular outcome data, long-term safety record, or physician-monitored treatment structure. Anyone currently on metformin should not switch without their doctor’s knowledge. “Can replace” is different from “is a reasonable alternative with physician oversight.”
What is the correct berberine dosage for blood sugar?
The dose used in most clinical trials showing significant blood sugar reduction is 500 mg three times daily before meals (1,500 mg/day total). This is also the dose most commonly compared to metformin. Phytosome formulations may achieve comparable effects at 500–600 mg/day due to higher bioavailability. Timing before meals is critical — take berberine 20–30 minutes before eating to maximize the alpha-glucosidase inhibition mechanism on post-meal glucose.
Does berberine lower HbA1c?
Yes — consistently across multiple meta-analyses. A 2022 systematic review of 37 RCTs (3,048 patients) found berberine reduced HbA1c by a weighted mean difference of −0.63% (P<0.001). In head-to-head trials vs. metformin, HbA1c reductions are comparable. Higher baseline HbA1c values are associated with larger reductions — people with worse blood sugar control tend to see more pronounced improvement.
Is berberine safe to take daily long-term?
Within the studied timeframe (up to 6 months in most trials), berberine appears safe with no serious adverse events reported across thousands of participants. Long-term safety data beyond 1 year is limited. The most documented concern is drug interactions via CYP450 enzyme inhibition — anyone taking prescription medications should discuss berberine with their doctor before starting. Annual liver function monitoring is a reasonable precaution for long-term use.
Can I take berberine with metformin at the same time?
Yes — and the combination has clinical support. A 2021 Italian RCT found adding berberine to existing metformin therapy reduced HbA1c by 7.5% and fasting glucose by 11.7% compared to metformin alone. The two compounds work through complementary mechanisms. However, combining them increases hypoglycemia risk, requires blood sugar monitoring, and should be done with your doctor’s awareness.
Does berberine have fewer side effects than metformin?
In the 2025 head-to-head prediabetes RCT, GI side effects occurred in 20% of berberine recipients vs. 30% in the metformin group — a meaningful difference. Standard berberine HCl can still cause GI discomfort (nausea, constipation, cramping), especially at higher doses. Phytosome formulations may reduce GI side effects further by improving absorption and leaving less unabsorbed berberine in the gut. Metformin extended-release (XR) also has fewer GI side effects than standard metformin.
Does berberine help with weight loss like metformin?
Both compounds modestly support weight loss in people with insulin resistance, primarily through improved metabolic efficiency rather than appetite suppression. Berberine shows lipid-lowering effects (LDL, triglycerides) beyond its blood sugar effects. The weight loss effects of both are modest and secondary to their primary mechanism — neither should be relied upon as a weight loss intervention in isolation.
What are the drug interactions with berberine?
Berberine inhibits CYP3A4 and CYP2D6 liver enzymes, affecting the metabolism of a wide range of medications. Clinically relevant interactions include: statins (increased statin blood levels → higher rhabdomyolysis risk), warfarin and other blood thinners, cyclosporine (immunosuppressant), some antidepressants (SSRIs), antifungal medications, and some cancer drugs. Anyone on multiple prescription medications should review their full medication list with a pharmacist or physician before starting berberine.
Is berberine FDA-approved for diabetes?
No. Berberine is classified as a dietary supplement in the United States and is not FDA-approved for the treatment or prevention of diabetes or prediabetes. It cannot be legally marketed with specific disease treatment claims on the label. This is a regulatory category distinction — it does not mean berberine is ineffective, but it does mean it lacks the safety and efficacy review process required for pharmaceutical approval. Prescription metformin has FDA approval and associated regulatory oversight that berberine does not.
The Bottom Line {#conclusion}
Berberine is not hype. Multiple meta-analyses across thousands of patients, and the most recent head-to-head RCT in prediabetes, confirm that berberine produces meaningful, statistically significant blood sugar reduction — comparable to metformin at equivalent doses, with fewer GI side effects in direct comparison.
The honest context: berberine is not metformin, and it can’t replace decades of cardiovascular outcome data or the physician-monitoring infrastructure that comes with prescription treatment. For people with prediabetes working on lifestyle-first management, or for metformin-intolerant patients looking for alternatives, berberine has genuine clinical support. For people already on metformin who want better blood sugar control, adding berberine as an adjunct — with their doctor’s knowledge — has the strongest evidence of all.
If you’re considering berberine, tell your doctor. Monitor your blood sugar. Use it before meals. Give it 12 weeks. And don’t mistake “equivalent short-term blood sugar outcomes” for “equivalent long-term disease management” — those are meaningfully different things.
This article is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider before making any changes to your diabetes or prediabetes management plan.
Written by Ethan Cole, Nutrition Expert | Meet Ethan →